Terms and Conditions
TOTAL WELLNESS CENTER – TERMS & CONDITIONS OF SERVICE
Version 11/25/25
TERMINOLOGY
“we”, “us”, “health provider”, “couselor”, “clinician”, “the practice”, “our team” refers to Total Wellness
Center or a person duly licensed and authorized to act on behalf of Total Wellness Center in relation to
the provision of the “services”.
“services” refers to any “psychiatric services” or treatment, including administrative work, either as
requested by you and/or delivered to you in accordance with all terms listed below.
“Psychiatric Services” refers to Psychiatric Diagnostic, Pharmacologic Management and Psychotherapy
to either for Individual, Couples, Group or Family.
“you”, “your”, “the patient”, refers to the person entering in this service agreement with Total Wellness
Center, either for your own or on the behalf of a person considered incapacitated by law and where you
are the lawful appointed guardian and/or has the power of attorney, and in either case, duly recognised
by the US courts.
“fee(s)”, “charge(s)”, “cost”, “copay”, “coinsurance” refers to any applicable cost to you in relation to
services rendered by us in accordance with this agreement.
1) ABOUT US
a) Total Wellness Center is a private outpatient mental health practice operating on a fee-for-service
model delivering Psychiatric services such as Assessments, Diagnosis, Medication Management
and Psychoterapy.
b) Our body of professionals are licensed to practice in New Jersey, New York and in Connecticut and
our services could be provided to you both in-person and/or online (Telemedicine) either at our
offices or via our secured and HIPPA compliant platform dependant of our providers’ availability.
c) You understand that Total Wellness Center does not provide emergency services. If an emergency
arises, you are directed to seek the nearest emergency room and/or call 911 for immediate medical
attention.
d) All services at Total Wellness Center are provided by appointment only, and we do not offer "walk-
in" services.
e) Ours offices are in:
New Jersey: 311 Claremont Avenue, Montclair, 07042
800 Catalpa Avenue, Teaneck, 07666
Connecticut: 76 Progress Drive, 235J, Stamford, 06902
f) Our postal address is:
PO Box 3189, Teaneck, New Jersey, 07666
g) Our patient HUB is open from Monday to Friday between 9am – 5pm (EST) except during national
holidays. Any communication received to our office outside of these hours will be attended in the
next working day.
Appointments & General Queries:
From 9am to 5pm on (973) 600-5465 option 2 or via booking@123psychiatry.com
Prescription support:
From 1pm to 5pm on (973) 600-5465 option 3 or via scripts2@123psychiatry.com
Billing support:
From 9am to 5pm on (973) 600-5465 option 4 or billing@123psychiatry.com
2) OUR SERVICES & PRACTICES
a) Your initial consultation with any member of our clinical team or providers serves as an evaluation
to determine your mental health needs and assess the most appropriate treatment for addressing
those needs. It is important to understand that these initial consultations do not guarantee that we
will provide treatment.
b) You understand that your mental health provider may make diagnostic and treatment
recommendations with which you may not agree (e.g., modality of treatment, duration of treatment,
frequency of visits, etc.) and that your provider may refer you to other clinicians outside of Total
Wellness Center who may be better able to address your concerns/needs. Again, you have the
right to refuse any such recommendations or referrals.
c) You will be able to discuss with your mental health provider clinical observations regarding the
presenting symptoms, issues, diagnosis or diagnoses, benefits/limitations of treatment, and
treatment interventions and expectations proposed, including risks and benefits to such treatments.
d) You understand that our providers do not complete any forms, letters, or other documentation until
the patient has completed at least six (6) months of continuous care with our practice. This
includes, but is not limited to: Disability forms (short-term, long-term, or state disability), FMLA
(Family and Medical Leave Act) paperwork, Return-to-work or fitness-for-duty letters, Letters for
emotional support animals (ESA), Letters for housing or workplace accommodations, Court-related
or legal documentation, Any third-party forms (e.g., insurance, employers, or schools).After six
months, it is at the provider’s sole discretion to determine whether the patient meets the clinical
criteria and whether sufficient documentation exists to support such requests. The decision will be
based on the provider’s clinical judgment, scope of practice, and ethical standards.
e) You will be given a clear description of the types of treatment recommended, such as
pharmacological treatment, individual counseling/therapy, group counseling/therapy, family/couples
counseling/therapy, addiction counseling, partial hospitalization, intensive outpatient programs, and
inpatient/outpatient treatment.
f) You understand that your mental health provider cannot guarantee results (e.g., less depressed,
improved marital satisfaction, etc.) of mental health services. However, you and your mental health
provider will identify clearly stated reasons, goals, and objectives for continuing/discontinuing
mental health treatment.
g) You understand that there may be some risks in participating in mental health services. These may
include, but are not limited to, addressing painful emotional experiences and/or feelings or being
challenged or confronted on a particular issue. Every effort will be made to maintain professional
integrity and appropriate treatment parameters and address mental health issues in a thoughtful
and respectful manner at all times with the ultimate goal always being to heal, treat, and overcome
mental health concerns/issues and re- establish health and wellness.
h) You are aware that you can discuss any risk, expected or unforeseen, versus its benefits with your
mental health provider at any time. In the case of psychiatric care, medications, side effects, and
alternative treatments can be discussed. Specific information regarding available research and
standards of practice for mental health treatment, for example during pregnancy and the
postpartum period, can also be discussed as part of your treatment plan. It is important to disclose
to your provider if YOU ARE PREGNANT, PLANNING TO GET PREGNANT OR
BREASTFEEDING, as some medications may be contraindicated and/or harmful during this time.
i) It is your responsibility to inform your heath provider of any known allergies, or any allergies that you
become aware after the commencement of your pharmacologic treatment as some medication
may cause serious adverse medical outcomes, including death.
j) Please inform our office after you have been seen and/or evaluated emergently, and we will
schedule a follow up outpatient appointment as soon as possible and/or clinically appropriate to
ensure continuity of your care.
k) We charge a processing/submission fee to obtain copies of medical records, in accordance with
state law. This fee is waived if the patient retrieves the records in person at our offices.
3) BILLING, FEES AND PAYMENTS
a) Total Wellness Center is a private outpatient mental health practice operating on a fee-for-service
model. We accept most major commercial insurances, as well as cash, debit/credit cards, and
check payments for services provided to you.
b) Unless specified and agreed to the contrary in advance, patients are expected to complete our
Credit Card Agreement (mandatory for phone sessions or telehealth appointments) during their
onboarding. Total Wellness Center does not hold your credit card details, instead, for security and
reassurance of our patients, we selected a Secure Payment Services Provider to handle all credit
card information through encrypted means. Your Credit Card will be safely stored and used on the
ad-hoc basis to pay for services either as a private/self-pay patient or as a patient using insurance
(co-pay, co-insurance, etc).
c) You must advise us of any changes to your credit card information, including to update any expired
card you may initially register. We may reserve the right to place your account in hold until your
credit card agreement is updated.
d) It is our policy and expectation that patients will pay their services at the time of service. However, if
a bill is generated, the bill is due immediately upon receipt.
e) You must inform the office immediately if you believe a charge made was incorrect or done in error.
Our office will investigate the matter if applicable, refund you any sum without delay.
f) If you are unable to attend your appointment, you must inform Total Wellness Center, during
business hours, at least 24 hours in advance of your scheduled time. If appointments are cancelled
with less than a 24-hour notice (LATE CANCELLATION) or if appointments are missed (NO-
SHOWS), a $75 becomes applicable to your account.
g) In the event that we are not able to directly collect our fees from you, we will issue you with an
invoice and a payment link. Any sum not paid within 30 days becomes overdue and may incur
additional fees. Total Wellness Center reserves the right to transfer any debt over 90 days to a debt
collection agency where you may be liable to additional fees.
PRIVATE PAY/SELF-PAY
h) All patients paying private fees are expected to pay in full at the time of service. Please refer to our
item 4 below (Our Rates) for an estimation of the fees associated with the services. Payments can
be made by check, cash, and/or credit/debit/HSA card at the time of service. We can also combine
various forms of payment if this is more convenient and/or preferred by the patient.
HEALTH INSURANCE PAY
i) Total Wellness Center and its providers are in-network with most major health insurance companies,
and we will bill those companies for the payment of services provided to you in accordance with
contracted agreement between those insurance companies and Total Wellness Center. If
applicable, we will also charge you any sum you are liable to as stipulated in your individual health
insurance policy (your benefits).
j) If you choose to use your health insurance, your benefits will need to be checked by our team prior
to your visit. We will ask you to provide a copy of your insurance card for our records. Once you
provide your insurance details, and prior to your appointment, we will verify on your behalf if our
practice is considered in-network or out-of-network with your insurance. We will also inform you
prior to your appointment, if your insurance company advises us of any co-pay, co-insurance or
deductible that you are liable to pay when using our services.
k) You must ensure your insurance is active so we can check your insurance benefits prior to your
visit. If a delay in providing your insurance information to us, impede us from carrying out the
necessary verification by the date of your visit, you will be liable to pay for the service in full as
outlined in section 4 (Our Rates). If your insurance is later verified to be active and we are able to
bill your insurance accordingly, we will be happy to refund, minus any fees applicable such as co-
pay, co-insurance or deductibles.
l) Total Wellness Center is not able to change the cost of co-pay, co-insurance, deductibles and out-of-
pocket limits.
m) Our office will submit claims to your insurance company in accordance with service provided to you
and in line with your benefit coverage. You must notify Total Wellness Center immediately
whenever there is any change to your health insurance coverage.
n) You are ultimately responsible for any charges not covered by your insurance company, including
but not limited to co-insurance, co-payments, deductibles, late cancellation and/or no-show fees.
o) You become immediately liable to pay for our services in full, as outlined in Section 4 (OUR
RATES), if your health insurance coverage is terminated or if your health insurance company
refuses to pay for any services that we provided to you (DENIED CLAIM).
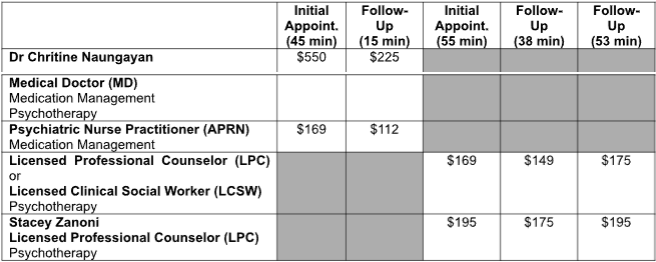
4) OUR RATES
a) The below rates apply to patients that are private/self-pay, becomes uninsured or where we are not
in network with the patient insurance.
b) These rates are periodically reviewed and subject to change, as determined by Total Wellness
Center. Total Wellness Center is committed to notify all patients in advance of such changes.
5) MEDICATION POLICY AND PRESCRIPTION REFILLS
BENZODIAZEPINE, STIMULANT, AND CONTROLLED SUBSTANCES
a) You understand that Total Wellness Center is involved in initiatives to decrease prescription related
deaths, including taking measures to limit the number of providers that will continue with their
prescription renewals to the same patient, in order to avoid patients having multiple prescribers of
controlled substances.
b) I am aware that the following medications are considered controlled substances [which include
benzodiazepines, sleep aids, and stimulants and may not be listed below]:
Adderall, Adderall XR, Adhansia XR, Adzenys XR-ODT, ALPRAZolam, Ambien, Ambien CR,
Amphetamine- Dextroamphet ER, Amphetamine-Dextroamphetamine, Ativan, Belsomra,
ClonazePAM, Concerta, Dexedrine, Dexmethylphenidate HCl, Dexmethylphenidate HCl ER,
Dextroamphetamine Sulfate, diazePAM, Evekeo, Evekeo ODT, Focalin, Focalin XR, KlonoPIN,
LORazepam, Lunesta, Methylin, Methylphenidate HCl, Methylphenidate HCl ER, Modafinil, Mydayis,
Phentermine HCl, Provigil, Restoril, Ritalin, Ritalin LA, Suboxone, Temazepam, Valium, Vyvanse,
Xanax, Xanax XR, Zaleplon, Zolpidem Tartrate.
c) In the event that your treatment plan, as suggested by your provider, will include the prescription
and intake of any controlled substances (including but not limited to the aforementioned ones), you
will, without fail, discuss the risks and benefits of being prescribed/administered this/these class[es]
of medication[s] as part of my treatment with my provider at Total Wellness Center before starting
to take such substances.
d) You agree to handle your medication responsibly and agree to take your medication only as
prescribed.
e) You will keep your medication in a safe place and will not share your medication with anyone else.
f) You agree to attend regular scheduled appointments with your provider in order to continue to
receive your medication refills and if you miss an appointment, you may not be able to receive a
refill until you are seen again by your provider, or a covering provider in his/her absence.
g) You will discuss the risks of being prescribed controlled substances (including the potential for
addiction, dependence, tolerance, withdrawal, abuse and misuse) with your provider.
h) You understand that taking this/these medication[s] outside of what has been prescribed or in
combination with alcohol or other illicit substances can result in serious adverse medical outcomes,
including death.
i) You agree on a treatment plan with your provider and agree to continue to have your response and
progress in treatment assessed on a regular basis.
j) If you have any questions or concerns during my treatment course, I will discuss them directly with
my provider.
k) You agree that your Medication Management provider and/or a covering nurse practitioner or
physician at Total Wellness Center will be the only prescribers of my psychotropic medications at
this time, including controlled substances, unless my provider and I discuss and agree otherwise
and document what other providers are involved in my care. I am also aware that my prescription
renewals are monitored by state prescription monitoring systems, which include New Jersey,
Connecticut, New York, Massachusetts and Pennsylvania, for the safety of patients and their
families, and that my provider and other physicians and providers at Total Wellness Center and
outside of Total Wellness Center can legally access this information in connection with prescribing
my medications.
l) You understand and agree that if you do receive controlled substance prescriptions outside of Total
Wellness Center after this agreement is in place, or violate the parameters discussed in this
agreement (i.e., consistently miss appointments, request early refills, lose or mishandle your
medication, etc.), Total Wellness Center may decide to have sufficient grounds for termination of
treatment at Total Wellness Center. Continued treatment can be discussed directly with my
provider, and if my provider is not comfortable continuing my care, referrals will be made at that
time for outpatient treatment clinics in my area.
PRESCRIPTION CHANGES AND REFILL REQUESTS
a) As some medication can only be refilled by your provider, we strongly advise you to schedule
your next appointment each time you meet with your provider, that helps to mitigate any
shortage due to lapse in scheduling appointments.
b) Should your encounter scheduling challenges eg your provider is on vacation, Total Wellness
Center will always offer covering providers to meet your needs, alternatively, depending on the
medication, our patient HUB may be able to ‘bridge’ a short gap (15 days maximum) until you
are able to see your preferred provider.
c) Total Wellness Center utilize electronic prescription writing for most medications. For the safety
of our patients, refill requests from pharmacies are not accepted.
d) To minimise any disruption in the provision of medication, you must inform us if you change your
pharmacy during the course of your treatment.
e) To minimize errors inherent in automated refill requests, we require patients to request refills
directly to their healthcare provider during their appointment, or if you need a refill before your
next scheduled appointment, to contact our patient HUB (Prescription Support).
f) Please note that any requests made during the weekends will be addressed on the following
Monday, or the subsequent business day in the event of a holiday. Please allow two business
days for turnaround time to handle refill requests. It is important that you do not wait until your
medication runs out to call us.
g) You understand that our providers may deem it necessary to have an encounter with you before
authorizing medication refills by phone, you may be required to speak with one of our clinicians
for an update on your medical and/or mental health condition.
h) If your prescription bottle indicates that you have refills remaining, you do not need to contact
our office. Instead, please contact your pharmacy, and they will refill it for you. However, if there
are no refills remaining at the pharmacy, you can then contact our office.
i) Please note that there are some prescriptions, such as controlled substances, that we cannot
refill over the phone. In such cases, our we may need to see you in our office before prescribing
medication for you.
j) If you need to discuss any changes to your current medication, you must schedule an
appointment and discuss this with your provider. The prescription support team cannot adjust or
alter your medication.
6) HIPAA & LIMITS OF CONFIDENTIALITY
a) You understand that the information that you share with your Mental Health Provider is confidential
and protected under the federal Health Insurance Portability and Accountability Act (HIPPA). This
law is intended to provide privacy standards to protect patients’ medical records and other
protected health information provided to, or created, maintained, used or disclosed by, health
plans, doctors, hospitals and other health care providers. It provides patients with access to their
medical records and more control over how their personal health information is used and
disclosed. It represents a uniform, federal floor of privacy protections for patients. State laws may
provide additional protections to patients with respect to their health information.
b) You understand that HIPAA allows Total Wellness Center to use and disclose your protected health
information without your specific written permission for coordinating services and delivering quality
care, including for payment, treatment and healthcare operations purposes. (Our Notice of Privacy
Practices can be found on: https://www.123psychiatry.com/wp-content/uploads/2024/05/
npp_booklet_hc_provider.pdf). These may include:
For Consultations and case conferences: with other providers at Total Wellness Center,
including staff who assist in facilitating patient information and care with clinicians.
For billing purposes: a diagnosis is given to your insurer for reimbursement purposes, medical
assistance and commercial insurance.
c) You understand, that in most cases, except as described below and in Item 6, paragraph b), your
confidential information cannot be released to another party without your written consent. However,
in certain circumstances, where required by law, we may be required to disclose otherwise
confidential information without your permission. These circumstances include:
Risk of Suicide: if you are assessed to be a danger to yourself; cannot guarantee your physical
safety against the intention of suicide; and/or have immediate suicidal plans, actions may be taken
to ensure your safety.
Risk of Harm: if you are assessed to be a danger to others; cannot guarantee their safety; and/or
have immediate, specific plans to cause fatal injury/harm to another person, actions may be taken
to protect the safety of others.
Court order/subpoena: If we receive a court order, subpoena, or other legal process requiring us
to disclose otherwise confidential information and/or records, your Mental Health Provider(s) may
be required to disclose such information/records. Mental Health Providers can also be subpoenaed
to testify in court without your consent.
Elderly and/or Child abuse/neglect: Your Mental Health Provider is required to report to the
appropriate authorities (i.e. Child Protective Services) any suspicion or evidence of past and
present child abuse or neglect.
Required by Law: We may be otherwise required by federal, state, or local law, statute, rule, or
order to disclose the information and/or records.
d) In the event that if you wish to have your records transferred or made available to another individual
or entity, or if you wish to have a family member or another person manage your account (e.g.
schedule appointments, request medication refills), you (or an authorized representative) are
required to need to sign a medical release authorizing us to do so. Such requests can be made by
contacting our patient HUB on (973) 600-5465 ext. 3 or via email to
medicalrecords@123psychiatry.com requesting a ‘Medical Release Form’.
e) You authorize Total Wellness Center to release/receive verbal and written information about me
to/from your medical insurance company and any referring physician. This authorization will end if I
give written instructions to Total Wellness Center to that effect, which I may do at any time.
7) TELEMEDICINE
a) You understand that Total Wellness Center offers psychiatry service both in-person and via
telemedicine. Patients will always have the choice to see a provider that best matches their
preferences. In the event that you decide to participate in a telemedicine consultation, this may be
provided by the Physicians (MD), Advanced Psychiatric Nurse Practitioners (APRN), Licensed
Professional Counselor (LPC) or a Licensed Clinical Social Worker (LCSW)of Total Wellness
Center, in connection with the following procedure(s) and/or service(s): Psychiatric Diagnostic
Examination with or without medical service, Pharmacologic management or Individual, Group and
Family psychotherapy
b) You understand and acknowledge that telemedicine is the use of electronic information and
communication technologies by a healthcare provider to deliver services to an individual when
he/she is located at a different site to the provider; and hereby consent to Total Wellness Center
clinical staff providing health care services to me via telemedicine.
c) You understand that the laws that protect the confidentiality of my protected health information, such
as HIPAA, also apply to telemedicine. As such, you understand that the information released by
me during a telemedicine session is confidential under such laws.
d) You understand that the same laws that may require my healthcare provider to disclose my
protected health information under certain circumstances also applies to information disclosed
through telemedicine.
e) You understand that, as always, your health insurance company may have access to my medical
records for quality review/audit. By agreeing to use telemedicine services, you consent Total
Wellness Center to share if required your protected health information with third parties as
permitted by law.
f) You understand and acknowledge that you are responsible for making the necessary arrangements
to obtain the necessary telecommunications devices (phone, tablet, computer etc.) and internet
access for the care and treatment provided by way of telemedicine.
g) You understand and acknowledge that you are solely responsible for the information security of the
communication devices which you will be utilizing for purposes of engaging telemedicine therapy,
and the means by which I am accessing the internet.
h) You acknowledge that Total Wellness Center cannot guarantee the security of any information that
you receive, store, or transmit on your chosen communication device(s).
i) You understand and acknowledge that Total Wellness Center takes your privacy very seriously, and
believes that my protected health information should remain protected. To that end, Total Wellness
Center has made reasonable arrangements to put into place HIPAA compliant security measures
which are designed to protect this information from any unwanted intrusions.
j) You understand and acknowledge that there are risks involved with telemedicine which may occur
despite the best and reasonable efforts of Total Wellness Center to guard my protected health
information, and the transmission of my personal information could be disrupted or distorted by
technical failures or interrupted by unauthorized persons.
k) You accept that Total Wellness Center cannot and does not make any representation that the
communication devices used by its patients meet its internal security standards. As such, it cannot
guard against the release of my personal and protected health information either through
unintentional dissemination or through the nefarious acts of others, which may be made possible
by security breaches on my own communications device.
l) You understand and acknowledge that you will be responsible for any copayments or coinsurance
that apply to my telemedicine visit, if not naturally covered by your health insurance policy.
m) You understand and acknowledge that you have the right to withhold or withdraw my consent to the
use of telemedicine in the course of your treatment at any time, without affecting my right to future
care or treatment for in-person appointments dependent of availability.
n) In such case, you must revoke my consent in writing at any time by contacting Total Wellness
Center patient HUB by either Fax (201) 353-2514 or via booking@123psychiatry.com.
o) You understand that you can chose to see your health provider in-person without having to revoke
your consent to telemedicine, however, if you do want exercise your right to revoke your consent to
telemedicine, this same service will not be made available to you until you have given in writing a
new consent to resume service.
p) You understand that it is your responsibility to have the appropriate consent in place when
requesting a telemedicine appointment with one of our health providers. If a telemedicine
appointment is made at your request, and if the appointment must later be cancelled due to the
absence of the appropriate consent, if this cancellation is made in less than 24-hour prior to the
appointment time, you may be charged a late cancellation fee as outlined in item 3, paragraph f) of
this agreement.
8) COMMUNICATION BY EMAIL, TEXT MESSAGE AND OTHER NON-SECURE MEANS
a) By entering in this service agreement with Total Wellness Center, you accept and may find it useful
to make contact to Total Wellness Center staff or the clinician team via email, text message (SMS)
or other electronic method of communication that, in their typical form, are not confidential means
of communication. Therefore, and likewise, Total Wellness Center may contact you or respond to
you via these same means to transmit the following protected health information as requested and
expected:
- Information related to the scheduling of meetings or other appointments
- Information related to billing and payment
- Acknowledgment of emails and phone calls received
- Other reports requested by you (which should be limited in nature and should include sensitive
information only when necessary)
b) You understand and accept that, there is a chance that a third party may be able to intercept and
eavesdrop on those messages. The kinds of parties that may intercept these messages include,
but are not limited to:
People in your home or other environments who can access your phone, computer, or other
devices that you use to read and write messages
Your employer, if you use your work email to communicate with Total Wellness Center staff and
clinician
Third parties on the Internet such as server administrators and others who monitor Internet
traffic.
c) You must consider if there are people in your life that may have access to your protected health
information, as per examples above, and take the necessary steps to mitigate this whenever
possible, such as in example, you may choose to stop communicating via a work email or chose
to/and limit communication with us to an specific communication method over another eg request
to only communicate via email and not via SMS.
d) You understand and give consent to Total Wellness Center to communicate limited protected health
information as described in Item 8, paragraph a) of this agreement.
e) You understand that you can revoke this consent to communicate your protected health information
via unsecure means at anytime. This request must be done in writing by either Fax (201) 353-2514
or via booking@123psychiatry.com.
f) You understand that it is your responsibility to have the appropriate consent in place when
communicating or requesting us to respond through unsecure means of communication and that
you may not receive any communication or response from us, through these same means until a
new consent is in place.
9) EMERGENCY CONTACTS AND DISCLOSE OF INFORMATION
a) In the event of an emergency and only in such event, I duly authorize Total Wellness Center to
contact any or all persons listed as my emergency contacts for the sole purpose of exchanging
information as authorized by me and registered on my intake form.
b) This authorization for release of information covers all past, present and future periods of
healthcare, includes healthcare provided by us or by others external providers, in the event that
you have authorized us to obtain and/or have provided us your historical medical information when
being treated by others.
c) I understand that this authorization will remain in effect until I either revoke it or submit a
subsequent written request for a change to our office either via
medicalrecords@123psychiatry.com, or via Fax Number (201) 353-2514 or via post to PO Box
3189, Teaneck, New Jersey, 07666.
d) I understand that a revocation is not effective to the extent that any person or entity has already
acted in reliance on my authorization or if my authorization was obtained as a condition of
obtaining insurance coverage and the insurer has a legal right to contest a claim.
e) I understand that my treatment, payment, enrolment, or eligibility for benefits will not be conditioned
on whether this authorization is revoked or if no authorization is given.
f) I understand that information used or disclosed pursuant to this authorization may be redisclosed by
the recipient and may no longer be protected by federal or state law.
10) TERMINATION OF SERVICES
TERMINATION BY YOU:
a) You can refuse any recommended treatment and terminate your treatment at any time. Notice of
termination is required in writing to either booking@123psychiatry.com or via post to PO Box
3189, Teaneck, New Jersey, 07666
b) You will not be charged for any psychiatric services after notifying us, however, you may still be
liable for any outstanding balance in your account for services provided to you prior to the
termination date. That includes, but not limited to, no-show fees or administrative work as
requested by you.
TERMINATION BY US:
c) Our clinicians reserve the right to refuse treatment to anyone if they do not feel it is appropriate to
engage in treatment or if it is not clinically indicated. In these instances, the clinicians will make
every effort to refer patients to the appropriate treatment facilities and/or providers who may be
better able to meet the patient’s mental health needs.
d) Patients who either reschedule, cancel or miss their appointments (NO SHOW) at least three times
within a six-month period (without a reasonable justification) are referred to another clinical office
outside our practice, which may be better suited to the patient’s schedule.
e) The entire team at Total Wellness Center work tirelessly to provide the best care to all our patients
and we will always operate in accordance with these terms and conditions, industry standards and
codes, local, state and federal laws. Total Wellness Center will not tolerate any conduct or
behaviour considered inappropriate, hostile, aggressive, threatening or of harassment nature. We
reserve the right and may terminate treatment to any person directly or indirectly associated with
such actions towards our team members.
f) As outlined in Item 5, paragraph l), Total Wellness Center reserves the right to terminate and
treatment whenever there are sufficient grounds to believe the medication or controlled substances
are being misused by the patient.